
CLASSIFYING ASTHMA SEVERITY AND INITIATING TREATMENT IN YOUTHS ≥ 12 YEARS OF AGE AND ADULTS
Assessing severity for patients who are not currently taking long-term control medications.
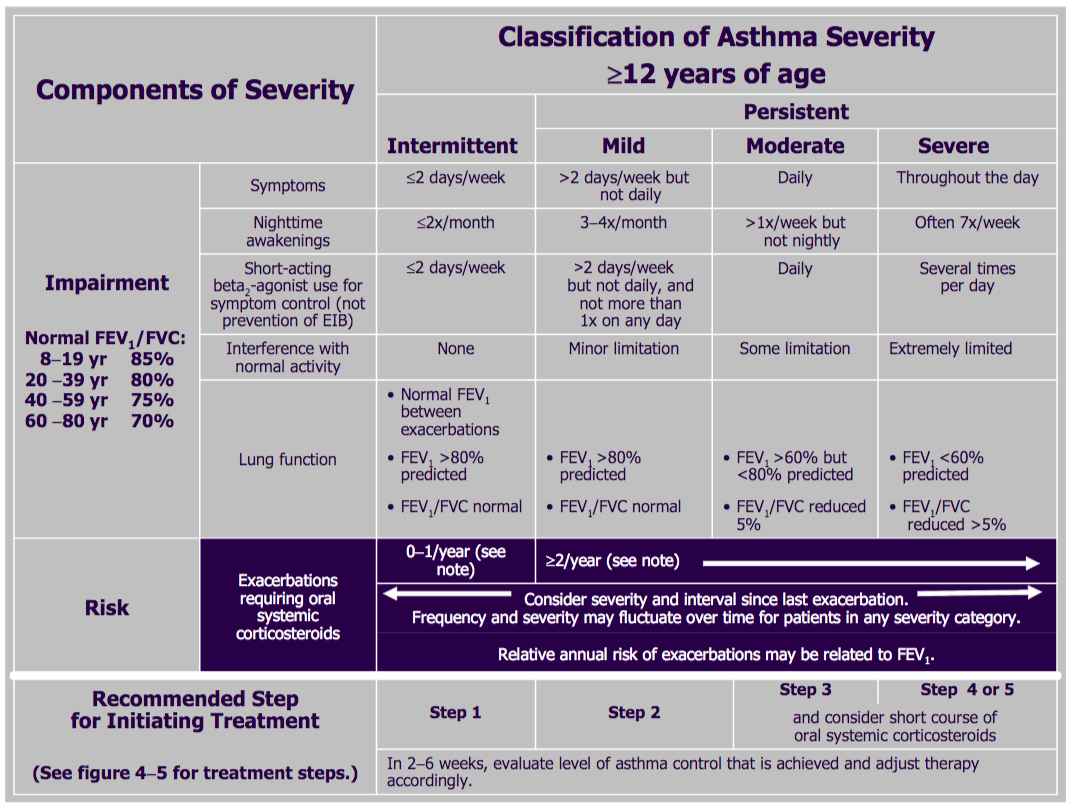
| Components of severity | Classification of asthma severity (≥12 years of age) | ||||
| Intermittent | Persistent | ||||
| Mild | Moderate | Severe | |||
| Impairment
Normal FEV1/FVC: 8 to 19 years 85 percent 20 to 39 years 80 percent 40 to 59 years 75 percent 60 to 80 years 70 percent |
Symptoms | ≤2 days/week | >2 days/week but not daily | Daily | Throughout the day |
| Nighttime awakenings | ≤2x/month | 3 to 4x/month | Weekly: >1x/week but not nightly | Often 7x/week (i.e. Often nightly) |
|
| Short-acting beta2-agonist use for symptom control (not prevention of EIB) | ≤2 days/week | >2 days/week but not daily, and not more than 1x on any day | Daily | Several times per day | |
| Interference with normal activity | None | Minor (mild) limitation | Some (moderate) limitation | Extremely (severely) limited | |
| Lung function | • Normal FEV1 between exacerbations
• FEV1 >80 percent predicted • FEV1/FVC normal |
• FEV1 ≥80 percent predicted
• FEV1/FVC normal |
• FEV1 >60 but <80 percent predicted
• FEV1/FVC reduced 5 percent |
• FEV1 <60 percent predicted
• FEV1/FVC reduced >5 percent |
|
| Risk | Exacerbations requiring oral systemic glucocorticoids | 0 to 1/year (see footnote) | ≥2/year (see footnote) | ||
| Consider severity and interval since last exacerbation | |||||
| Frequency and severity may fluctuate over time for patients in any severity category | |||||
| Relative annual risk of exacerbations may be related to FEV1 | |||||
| Recommended step for initiating treatment | Step 1 | Step 2 | Step 3 | Step 4 or 5 | |
| And consider short course of oral systemic glucocorticoids | |||||
| In two to six weeks, evaluate the level of asthma control that is achieved and adjust therapy accordingly. | |||||
Image of above table from NIH.gov: Classification of Asthma Severity
{kind=link}
The level of severity is determined by assessment of both impairment and risk. Assess impairment domain by patient’s/caregiver’s recall of previous two to four weeks and spirometry. Assign severity to the most severe category in which any feature occurs. At present, data are inadequate to correlate frequencies of exacerbations with different levels of asthma severity. In general, more frequent and intense exacerbations (eg, requiring urgent, unscheduled care, hospitalization, or ICU admission) indicate greater underlying disease severity. For treatment purposes, patients who had ≥2 exacerbations requiring oral systemic glucocorticoids in the past year may be considered the same as patients who have persistent asthma, even in the absence of impairment levels consistent with persistent asthma.
FEV1: forced expiratory volume in one second; FVC: forced vital capacity; ICU: intensive care unit.
STEPWISE APPROACH FOR MANAGING ASTHMA IN YOUTHS ≥ 12 YEARS OF AGE AND ADULTS

Key: Alphabetical order is used when more than one treatment option is listed within either preferred or alternative therapy. EIB, exercise-induced bronchospasm; ICS, inhaled
corticosteroid; LABA, long-acting inhaled beta2-agonist; LTRA, leukotriene receptor antagonist; SABA, inhaled short-acting beta2-agonist
Notes:
corticosteroid; LABA, long-acting inhaled beta2-agonist; LTRA, leukotriene receptor antagonist; SABA, inhaled short-acting beta2-agonist
Notes:
- The stepwise approach is meant to assist, not replace, the clinical decision-making required to meet individual patient needs.
- If alternative treatment is used and response is inadequate, discontinue it and use the preferred treatment before stepping up.
- Zileuton is a less desirable alternative due to limited studies as adjunctive therapy and the need to monitor liver function. Theophylline requires monitoring of serum concentration levels.
- In step 6, before oral systemic glucocorticoids are introduced, a trial of high-dose ICS + LABA + either LTRA, theophylline, or zileuton may be considered, although this approach has not been studied in clinical trials.
- Step 1, 2, and 3 preferred therapies are based on evidence A; step 3 alternative therapy is based on evidence A for LTRA, evidence B for theophylline, and evidence D for zileuton. Step 4 preferred therapy is based on evidence B, and alternative therapy is based on evidence B for LTRA and theophylline and evidence D for zileuton. Step 5 preferred therapy is based on evidence B. Step 6 preferred therapy is based on (EPR-2 1997) and evidence B for omalizumab.
- Immunotherapy for steps 2 to 4 is based on evidence B for house dust mites, animal danders, and pollens; evidence is weak or lacking for molds and cockroaches. Evidence is strongest for immunotherapy with single allergens. The role of allergy in asthma is greater in children than in adults.
- Clinicians who administer immunotherapy or omalizumab should be prepared and equipped to identify and treat anaphylaxis that may occur.
The above is reproduced from http://www.nhlbi.nih.gov/files/docs/guidelines/09_sec4_lt_12.pdf
Additional Sources:
- National Heart, Lung, and Blood Institute: http://www.nhlbi.nih.gov/health-pro/guidelines/current/asthma-guidelines/full-report
- AAFP, Overview of Asthma