
Causes of Secondary Hypertension: ABCDEF
- Apnea (OSA), Adrenals (aldosteronism), Accuracy of diagnosis.
- Bruit and Bad kidneys. Bruits come from blood vessel narrowing (RAS). Bad kidneys (glomerular disease & renal parenchymal disease).
- Catecholamines, Cushing’s sydrome, and coarctation of the aorta.
- Drugs (Medications and illicit drugs)
- Endocrine disorders or Erythropoietin
- Food or diet.
See this AFP article for the mnemonic.
RAS = Renal artery stenosis
| Cause | Suggestive clinical features | Workup |
| Renovascular disease | An acute elevation in serum creatinine of at least 30% after administration of ACE) inhibitor or an ARB. Moderate to severe HTN in a patient with diffuse atherosclerosis, a unilateral small kidney, or asymmetry in renal size of more than 1.5 cm that cannot be explained by another reason. Moderate to severe HTN in patients with recurrent episodes of flash pulmonary edema. An onset of stage II HTN after age 55 yrs Abdominal bruit (not very sensitive). |
For the initial testing start with either: 1) U/S (duplex Doppler U/S), 2) CTA, 3) MRA depending on local availability, expertise, and the presence or absence of renal insufficiency. There is little value and potential harm from radiologic testing if the patient is not a candidate for a corrective procedure. Because of the potential for harm from invasive procedures, test only patients who have a high likelihood of benefiting from the procedure. |
| Primary renal disease (Parenchymal disease) | High serum creatinine Abnormal UA |
UA, urine creatinine, work up the cause of parenchymal kidney disease. |
| Pheochromocytoma | The classic triad of symptoms in patients with a pheochromocytoma consists of episodic headaches (usually pounding), sweating, and tachycardia (w/ palpitations). | Measure 24-hr urinary fractionated metanephrines & catecholamines or plasma fractionated metanephrines.
If there is a low index of suspicion for pheochromocytoma, get a 24-hour urinary fractionated catecholamines and metanephrines; if there is a high index of suspicion, get plasma fractionated metanephrines. Use an algorithm like this one from uptodate.com Nmet: normetanephrine; Met: metanephrine. |
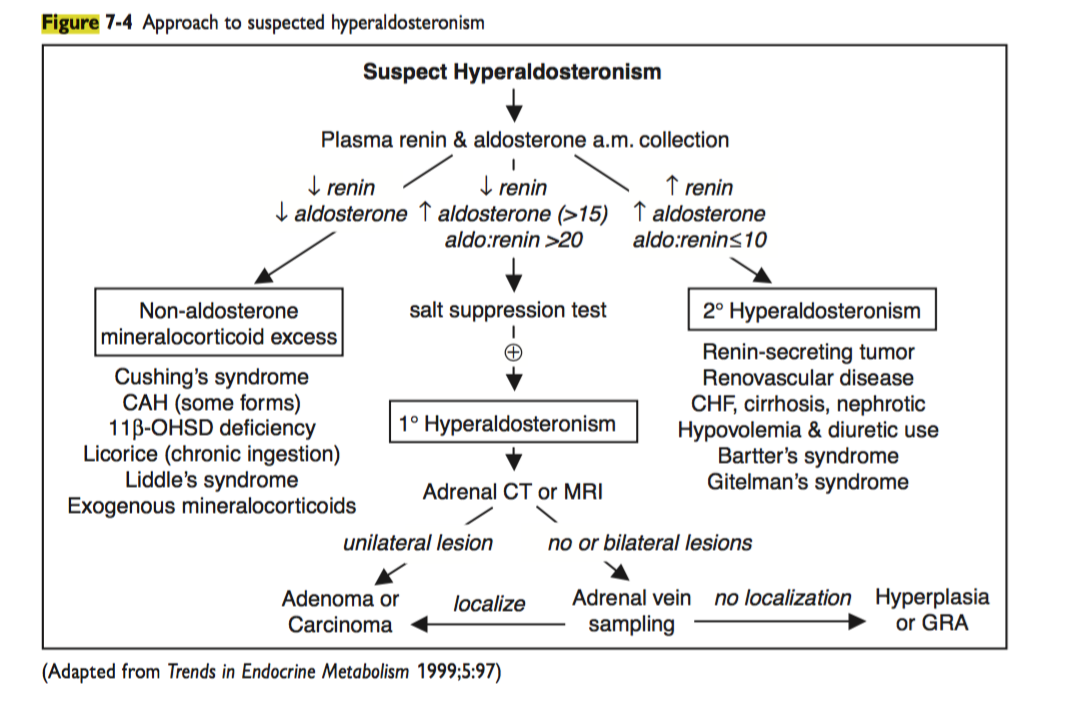
| Primary aldosteronism | Unexplained hypokalemia with urinary potassium wasting; however, more than one-half of patients are normokalemic | Start with: Peripheral aldosterone concentration (PAC) and peripheral renin activity (PRA), preferably after being up for 2 hours, are the preferred screening tests for hyperaldosteronism. A high PAC> 15 ng/dl and a PAC/PRA ratio of >20 suggests an adrenal cause. If PAC/PRA is abnormal, an aldosterone suppression test should be ordered. Follow the approach in pocket medicine or another resource. |
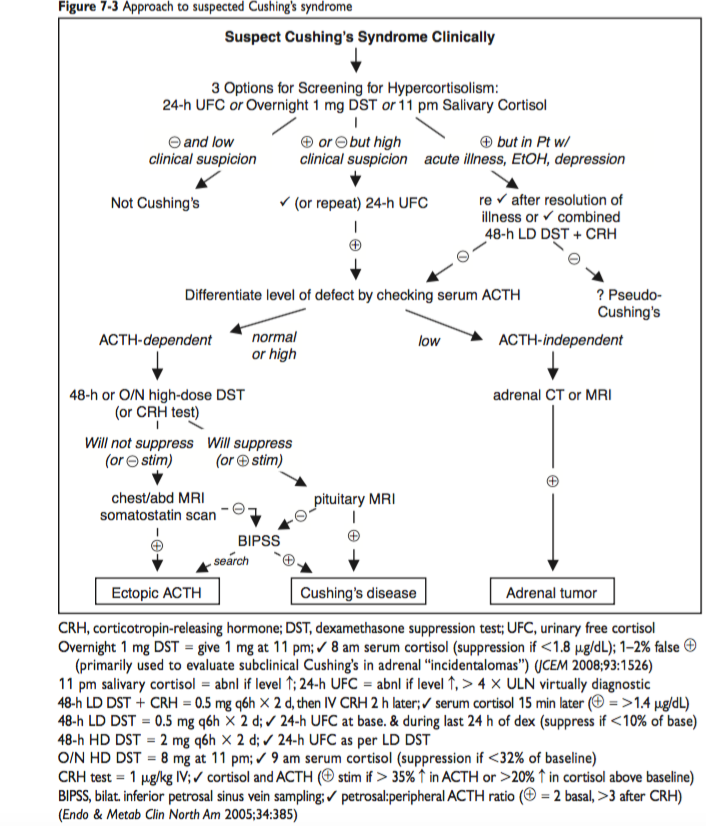
| Hypercortisolism (Cushing’s syndrome) | Cushingoid facies, central obesity, proximal muscle weakness, and ecchymoses.
May have a history of glucocorticoid use |
3 options for screening for hypercortisolism: > 24-hr urinary free cortisol (UFC) or > 1 mg Dexamethasone Suppression Test (DST), or > 11 p.m. salivary cortisol. Then follow the approach in pocket medicine or another resource. |
| Obstructive Sleep apnea. | Primarily seen in obese men who snore loudly while asleep. Daytime somnolence, fatigue, and morning confusion. |
In-laboratory polysomnography or home sleep apnea testing.
OSA: obstructive sleep apnea; AHI: apnea-hypopnea index. Follow uptodate.com approach or one from another resource. Read this uptodate article |
| Coarctation of the aorta. | Hypertension in the arms with diminished or delayed femoral pulses and low or unobtainable blood pressures in the legs. Left brachial pulse is diminished and equal to the femoral pulse if the origin of the left subclavian artery is distal to the coarctation. |
The clinical dx of coarctation of the aorta is based upon the characteristic findings of systolic hypertension in the upper extremities, diminished or delayed femoral pulses (brachial-femoral delay), and low or unobtainable arterial blood pressure in the lower extremities. The diagnosis is confirmed by noninvasive imaging methods, particularly echocardiography.
MRA or CTA clearly defines the location and severity of coarctation of the aorta, as well as collateral vessels |
| Primary hyperparathyroidism | Elevated serum calcium | |
| Hypothyroidism Hyperthyroidism |
Symptoms of hypothyroidism | Check TSH. If elevated, check free T4 |
| Drugs -Oral contraceptive pills, -NSAIDs, -Stimulants (e.g. cocaine, methylphenidate), -Calcineurin inhibitors, -Antidepressants |
New elevation in blood pressure temporally related to use |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
OSA=Obstructive sleep apnea; RAS=Renal Artery Stenosis (Renovascular disease); COA=Coarctation of the aorta. Primary aldosteronism = Conn’s syndrome
Alternative presentation: Adrenals and Kidneys; Breathing problems (OSA); Coarctation of the aorta; Drugs; Endorine, Food and diet.
Reference
http://www.aafp.org/afp/2017/1001/p453.html
http://www.aafp.org/afp/2010/1215/p1471.html
Uptodate.com