
“The cause of hyponatremia can be determined in part by how the patient’s kidneys are responding to the condition. If the urine is appropriately dilute, then the most likely cause of hyponatremia is excessive water intake or inadequate solute intake. Conversely, if the urine is concentrated, the patient may be hypovolemic or have the syndrome of inappropriate secretion of antidiuretic hormone (SIADH). The relative volume of the patient’s extravascular fluid will help determine how to proceed with treatment. Spot urine sodium or serum uric acid levels can be used to help ascertain whether the patient is hypovolemic, euvolemic, or hypervolemic.
No treatment specific to hyponatremia is required when the serum osmolality is either normal or elevated. Both iso-osmolar hyponatremia and hyperosmolar hyponatremia are due to an overabundance of another osmole such as glucose, mannitol, or contrast dye. These situations are often referred to as pseudohyponatremia.” The ABFM
Below, I make explanatory marks on a portion of a hyponatremia algorithm from the AAFP. The original algorithm is here.
{kind=link}
Click here to view a larger version of the hypotonic hyponatremia diagram below.
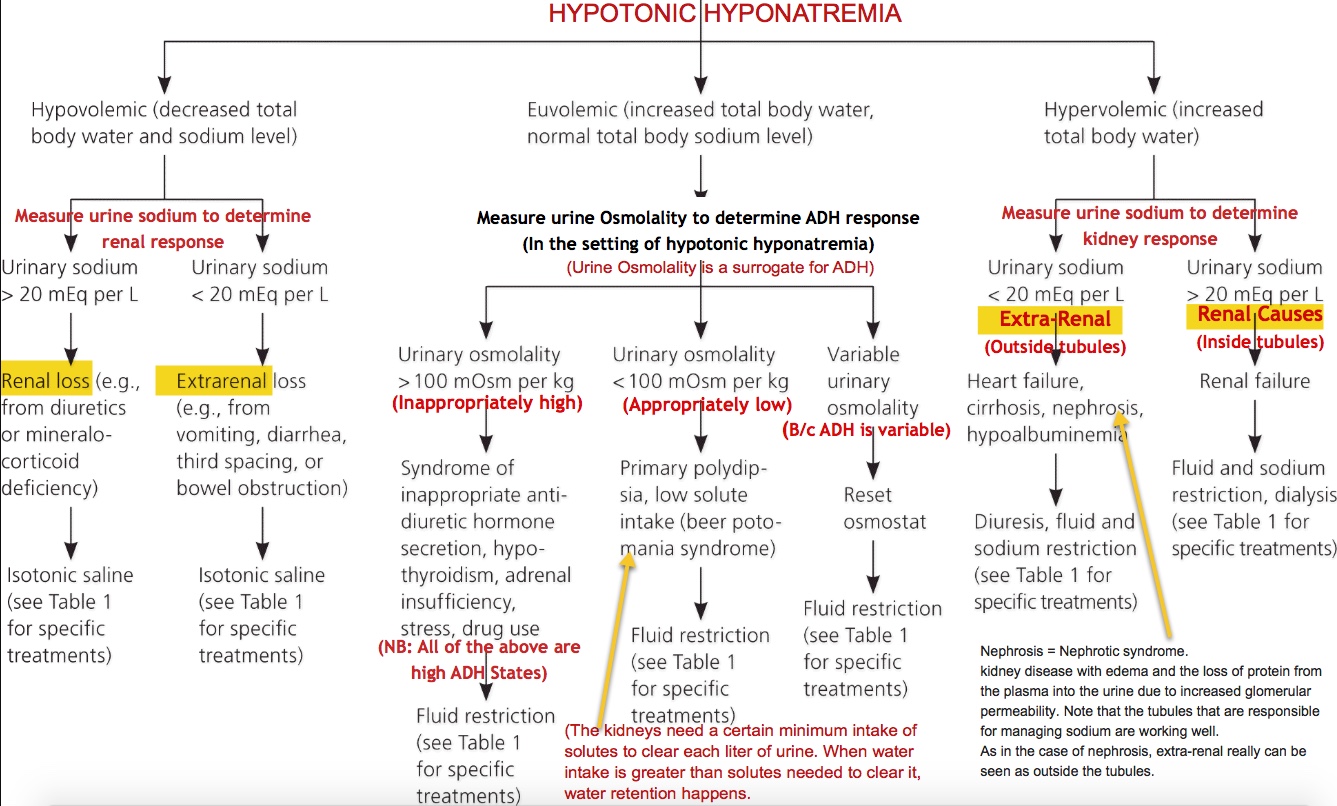{kind=link}
