
Proximate cause: Excess of water in relation to sodium. It can be induced by 1) taking in too much water (e.g. primary polydipsia) and/or by 2) impaired water excretion (e.g. due, to advanced renal failure) or by 3) persistent release ADH. “Hyponatremia is almost always due to increased ADH“.
H&P Performed.
Eval for volume status on PE.
Initial labs:
– CMP1, serum osmolality, urinary sodium conc., urine osmolality.
-TSH, adrenal function (if applicable)
Reviewed steps for workup of hyponatremia.
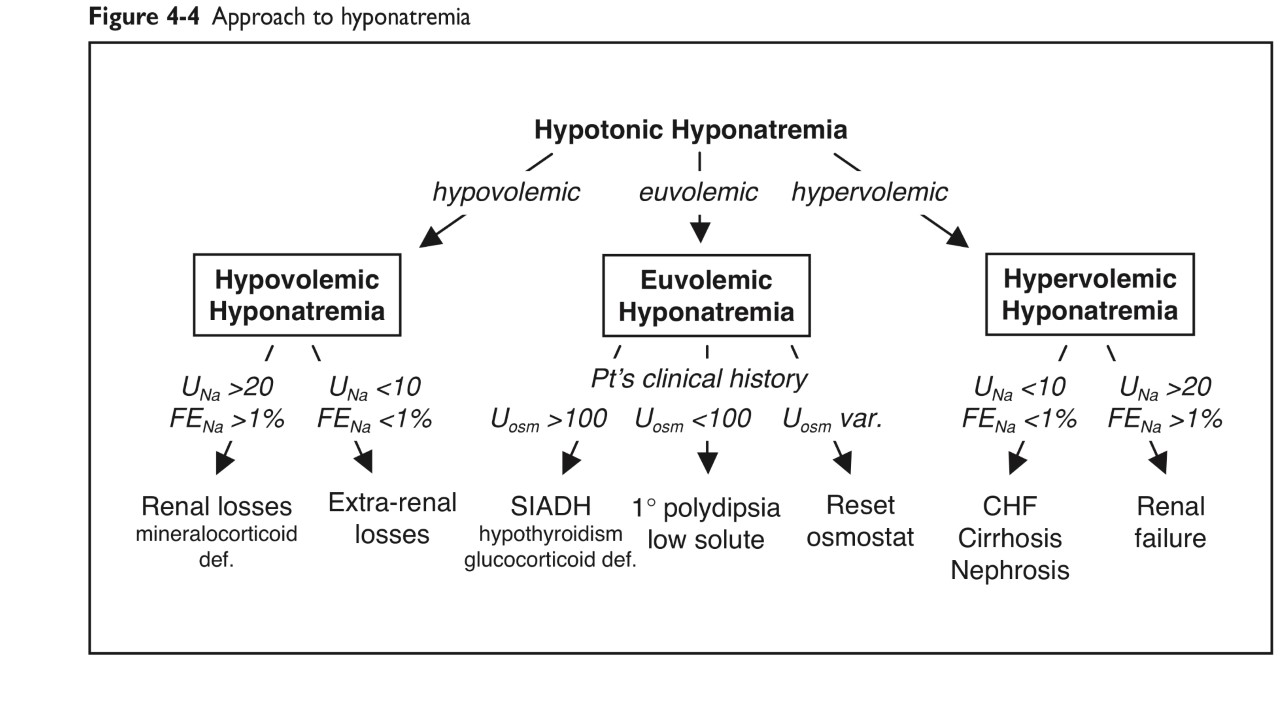
Reviewed Hyponatremia Algorithm.
Will determine cause of hyponatremia.
{kind=link}
Treatment
Asymptomatic chronic hyponatremia: correct sodium conc. at a rate of ≤0.5 mEq/L/h; the goal of initial tx is to raise the serum sodium conc. by 4 to 6 mEq/L in a 24-hour period. Max. of 8mEq/L in 24hrs2. This is to avoid osmotic demyelination syndrome (ODS). See asymptomatic hyponatremia.
Asymptomatic acute hyponatremia: same goal as for chronic but can be achieved faster.
Symptomatic (severe) hyponatremia (acute or chronic): Treat severe symptomatic hyponatremia with hypertonic 3% saline infused at a rate of 0.5 to 2 mL per kg per hour until symptoms resolve. “The rate of sodium correction should be 6 to 12 mEq per L in the first 24 hours and 18 mEq per L or less in 48 hours.” AAFP 2015
Key points
- Workup of Hyponatremia.
- Determining the Cause of Hyponatremia.
- Causes of SIADH.
- Hyponatremia Algorithm from the AAFP 2015, great algorithm (see link to article in reference)
- Principles and Pathophysiology of Sodium and Water Homeostasis.
- Classifying Hyponatremia by Symptoms and Sodium Concentration.
- True Hyponatremia Classified by Volume Status.
- Determining the Cause of Hyponatremia.
- Urine sodium tells us how the kidneys are doing. It is used to distinguish between renal and extra-renal causes of hyponatremia.
- Urine Osmolality tells us how ADH is acting on the kidneys (affecting its concentrating or diluting ability) in the context of the current plasma sodium and plasma osmolality. Is the ADH response appropriate? Inappropriate?
- MedCalc: Hyponatremia & Hypernatremia, calculator for both hyponatremia and hypernatremia (recommended in Pocket Medicine)
- Excellent Article from AAFP, 2015: Diagnosis and Management of Sodium Disorders: Hyponatremia and Hypernatremia
- Algorithm for Hypotonic Hyponatremia from Pocket Medicine, 4th Edition
{kind=link}
Hypovolemic, euvolemic-, and hypervolemic hyponatremias
Hypertonic saline, 3% normal saline is only given in the ICU and you need a central line to give it.
If hypervolemic: Consider a daily dose of Lasix 40-80IV if giving a lot of NS.
Notes
1 CMP give us sodium & other electrolytes, glucose, and creatinine.
2 Different sources cite different rates of correction. The AFFP 2015 article below says, “Chronic hypernatremia should be corrected at a rate of 0.5 mEq per L per hour, with a maximum change of 8 to 10 mEq per L in a 24-hour period”
Read this uptodate.com article.
References
- Sahay M, Sahay R. Hyponatremia: A practical approach. Indian Journal of Endocrinology and Metabolism. 2014;18(6):760-771. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4192979
- Am Fam Physician. 2015 Mar 1;91(5):299-307. Diagnosis and Management of Sodium Disorders: Hyponatremia and Hypernatremia. https://www.aafp.org/afp/2015/0301/p299.html
- Lee JJY, Kilonzo K, Nistico A, Yeates K. Management of hyponatremia. CMAJ : Canadian Medical Association Journal. 2014;186(8):E281-E286.
- Hyponatraemia Explained Clearly On Youtube by MedCram.com.
- The rest of Medcram.com hyponatremia series.